Vasectomy: A Comprehensive Guide to the Permanent Male Contraceptive
Introduction: A Definitive Choice in Family Planning
Vasectomy stands as one of the most effective, safe, and permanent methods of contraception available. It is a deliberate, elective surgical procedure that provides a reliable endpoint to male fertility, offering couples freedom from other contraceptive concerns. Despite its high efficacy and low complication rate, vasectomy is often shrouded in myths regarding its impact on masculinity, sexual function, and health. Modern vasectomy is a minimally invasive, outpatient procedure grounded in decades of refinement. This guide provides a detailed, evidence-based exploration of the procedure, its implications, and the considerations essential for informed decision-making.
Part 1: What is a Vasectomy? The Science of Sterilization
A vasectomy is a surgical sterilization procedure for men. Its goal is to interrupt the pathway sperm take from the testicles to the semen.
Anatomy & Physiology: Sperm are produced in the testicles and mature in the epididymis. They then travel through a tube called the vas deferens (one on each side), which carries them to the urethra to be ejaculated.
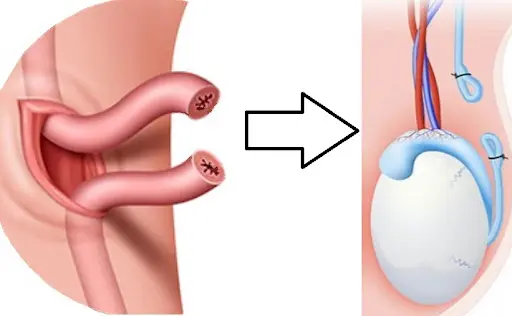
The Procedure’s Core: During a vasectomy, a small segment of each vas deferens is cut, sealed, or occluded. This prevents sperm from entering the seminal fluid. Importantly:
Testosterone production in the testicles is unaffected. Hormone levels, libido, and male characteristics remain unchanged.
The volume of ejaculate is minimally reduced (sperm constitute only ~5% of semen volume). Most men notice no difference.
Sperm production continues, but the sperm are reabsorbed by the body naturally.
Part 2: The Consultation: Making an Informed Decision
A thorough pre-vasectomy consultation with a urologist or family medicine physician is mandatory. This visit ensures the procedure is appropriate and that the patient understands it is considered permanent.
Key Discussion Points:
Permanence: Vasectomy reversal is possible but is a more complex, expensive microsurgery with variable success rates that decline over time. It should not be factored into the initial decision.
Alternatives: Review all other contraceptive options (condoms, female sterilization, IUDs, hormonal methods).
Motivation: Is the decision mutual and free from coercion? Is the family complete?
“What-If” Scenarios: Discuss future life changes (new partner, death of a child) that might alter feelings about fertility.
Medical History: Review bleeding disorders, anatomical issues (e.g., undescended testicles), or chronic scrotal pain.
Ideal Candidate: A man who is certain he does not desire future biological children, is in a stable relationship with mutual agreement, and understands the procedure’s permanence.
Part 3: The Procedure: Techniques and What to Expect
Modern vasectomy is typically a 15-30 minute outpatient procedure performed under local anesthesia in a clinic or office procedure room.
Pre-Procedure Preparation:
Shave or clip scrotal hair.
Arrange for transportation home.
Take a prescribed anti-anxiety medication if offered.
Bring supportive underwear (like a jockstrap).
Surgical Techniques – Two Primary Methods:
Conventional Incision Vasectomy:
One or two small incisions (about 1 cm) are made in the upper scrotum.
Each vas deferens is isolated, a segment is removed, and the ends are sealed.
Sealing Methods: Suture ties, cauterization (thermal sealing), or a combination. Fascial interposition—placing a tissue layer between the cut ends—is often used to further reduce failure risk.
No-Scalpel Vasectomy (NSV) – The Gold Standard:
This is not “incision-less,” but it is minimally invasive.
The surgeon uses a specialized sharp, pointed hemostat to make a single, tiny puncture in the scrotal skin.
The vas is gently elevated through this puncture, isolated, and sealed.
Advantages: Less bleeding, smaller wound, reduced post-operative pain, faster healing, lower risk of infection.
During the Procedure: Patients are awake but numb. Sensations of pulling or pressure are common, but sharp pain should be reported immediately.
Part 4: Recovery and Post-Operative Care
Proper aftercare is crucial for comfort and to prevent complications.
The First 48-72 Hours (The Critical Period):
REST. Limit all activity. The goal is to minimize swelling.
Ice: Apply ice packs to the scrotum (20 minutes on, 20 minutes off) to reduce swelling and pain.
Support: Wear a jockstrap or tight-fitting briefs 24/7 for at least a week for comfort and to limit movement.
Pain Management: Use prescribed or over-the-counter analgesics (e.g., acetaminophen, ibuprofen).
The First Week:
Avoid heavy lifting (>15-20 lbs), strenuous exercise, and sexual activity.
Most men can return to sedentary work within 1-2 days.
Longer-Term:
Gradual return to exercise after 1 week. Full contact sports may require 2-4 weeks.
Sexual activity can usually be resumed after 7 days, or when comfortable.
Part 5: The Most Critical Phase: Post-Vasectomy Semen Analysis (PVSA)
A vasectomy is NOT immediately effective. Sperm remains in the vas deferens beyond the surgical site. It takes time and ejaculations (typically 15-20) to clear the pipeline.
Protocol: The standard is to provide a semen sample for analysis at least 3 months after the procedure.
The Goal: Two consecutive semen samples showing azoospermia (zero sperm).
Success: Only after receiving formal clearance from the doctor is the vasectomy considered successful, and alternative contraception can be safely discontinued.
Rare Findings: “Non-motile sperm” may be present; guidelines exist for this scenario. Persistent motile sperm indicates a procedural failure.
Effectiveness: Once cleared, vasectomy is >99% effective at preventing pregnancy, making it one of the most reliable contraceptive methods known.
Part 6: Risks, Complications, and Myths Debunked
Potential Complications (Rates are low with an experienced surgeon):
Early (Short-Term):
Bruising/Hematoma (1-2%): Blood collection in the scrotum. Usually resolves with time.
Infection (<1%): Treated with antibiotics.
Sperm Granuloma (10-30%): A small, sometimes tender lump at the surgery site where sperm leak and cause inflammation. Most are asymptomatic.
Late (Long-Term):
Chronic Scrotal Pain (Post-Vasectomy Pain Syndrome – PVPS): The most debated complication. Defined as bothersome pain lasting >3 months. Incidence estimates vary widely (1-15%). Most cases are mild and manageable; severe, disabling pain is rare (<1%).
Failure (Recanalization): ~1 in 2,000 risk. Usually occurs early; late failure is exceedingly rare.
No Increased Risk is conclusively linked to prostate cancer, heart disease, or other systemic illnesses.
Myths vs. Reality:
Myth: It causes erectile dysfunction or loss of libido.
Myth: It’s a major, castrating surgery.
Myth: It changes the feeling of orgasm or ejaculation.
Part 7: Ethical and Social Considerations
Vasectomy represents a significant shift in contraceptive responsibility, which has historically fallen disproportionately on women. It offers couples a highly effective option that:
Decouples contraception from sexual activity.
Is less invasive and carries lower overall risk than female sterilization (tubal ligation).
Requires a mature, collaborative decision within a partnership.
Conclusion: A Permanent Step, Taken Confidently
Vasectomy is a powerful tool in family planning for the man who is certain his journey of biological fatherhood is complete. Its success hinges on informed consent, a skilled surgeon using modern techniques, and strict adherence to post-operative clearance protocols. By demystifying the procedure and confronting myths with scientific evidence, men can approach this decision with clarity and confidence. For the right individual, it offers a lifetime of contraceptive freedom, contributing to relationship stability and personal autonomy.
Resources for Further Information:
American Urological Association (AUA): Vasectomy Guidelines.
Planned Parenthood: Provides vasectomy services and education.
Urology Care Foundation: Patient-friendly materials.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice. The decision to undergo a vasectomy should be made in consultation with a qualified healthcare provider who can address individual circumstances and risks.