Mesothelioma: A Comprehensive Guide to the Asbestos-Linked Cancer
Introduction: A Legacy of Exposure, A Modern Diagnostic Challenge
Mesothelioma is a rare, aggressive, and universally fatal cancer that arises from the mesothelial cells lining the body’s internal cavities. Its defining characteristic is its overwhelmingly strong link to asbestos exposure, with approximately 80% of cases directly attributable to this single environmental and occupational carcinogen. Unlike most cancers, mesothelioma has an exceptionally long latency period—typically 20 to 50 years—between initial asbestos exposure and clinical diagnosis. This delay means that today’s patients are often suffering from exposures that occurred decades ago, in industries like shipbuilding, construction, insulation, and manufacturing. The disease is a master of mimicry, presenting with vague symptoms that often lead to delayed diagnosis at an advanced stage, when curative options are limited. This guide provides a detailed exploration of mesothelioma’s types, causes, diagnostic complexity, and the evolving landscape of treatment.
Part 1: Understanding the Disease – Types and Anatomy
Mesothelioma is categorized by the location in the body where it originates.
1. Pleural Mesothelioma (80-90% of cases):
Location: Develops in the pleura, the thin membrane lining the chest cavity and surrounding the lungs.
Presentation: Causes symptoms related to the lungs and chest wall, such as shortness of breath and chest pain.
Progression: The tumor grows, thickens the pleura, and can encase the lung (a “rind” of tumor), leading to progressive lung compression and respiratory failure.
2. Peritoneal Mesothelioma (10-20% of cases):
Location: Originates in the peritoneum, the membrane lining the abdominal cavity and organs.
Presentation: Causes abdominal pain, swelling (ascites), nausea, and bowel obstruction.
Prognosis: Historically poor, but has seen improved outcomes with aggressive multimodal treatment.
3. Rare Forms (<1% each):
Pericardial Mesothelioma: In the sac surrounding the heart. Causes constrictive pericarditis, heart failure.
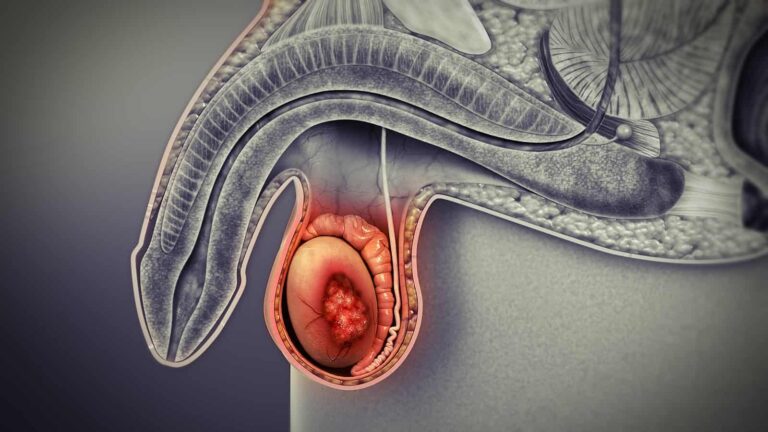
Testicular (Tunica Vaginalis) Mesothelioma: In the lining of the testicle. Presents as a testicular mass or hydrocele.
Part 2: The Unavoidable Cause – Asbestos and Pathogenesis
Asbestos is a naturally occurring, fibrous silicate mineral prized for its heat resistance and durability. When disturbed, it releases microscopic, needle-like fibers into the air.
Mechanism of Damage: When inhaled or ingested, these asbestos fibers penetrate deep into tissues. They are physically durable and biopersistent—the body cannot break them down or expel them effectively.
Chronic Inflammation & Carcinogenesis: The trapped fibers cause chronic inflammation, oxidative stress, and direct physical damage to DNA over decades. This persistent injury eventually leads to malignant transformation of mesothelial cells. Key genetic alterations involve tumor suppressor genes like BAP1, NF2, and CDKN2A.
No Safe Exposure Level: While heavy, prolonged occupational exposure carries the highest risk, cases have been documented from secondary exposure (e.g., washing the clothes of a worker) and even environmental exposure near natural deposits or industrial sites.
Other Potential Risk Factors (Much Less Common):
Zeolites: Erionite, a mineral fiber similar to asbestos, found in certain geographic regions (e.g., Turkey).
Radiation: Prior radiation therapy to the chest or abdomen.
SV40 Virus: Historical contamination of polio vaccines; its role remains controversial and unproven as a causative agent.
Part 3: Clinical Presentation – Vague Symptoms and Diagnostic Delay
Symptoms are insidious, non-specific, and often attributed to more common conditions like pneumonia, COPD, or irritable bowel syndrome.
Pleural Mesothelioma Symptoms:
Shortness of Breath (Dyspnea): Due to pleural effusion (fluid buildup) or tumor restricting lung expansion.
Persistent, Dull Chest Wall Pain: Often unilateral. Pain may radiate to the shoulder or upper abdomen.
Dry, Hacking Cough.
Unexplained Weight Loss and Fatigue.
Clubbing of Fingers (late sign).
Peritoneal Mesothelioma Symptoms:
Abdominal Pain and Swelling (Ascites).
Early Satiety and Nausea.
Bowel Habit Changes or Obstruction.
Unexplained Weight Loss.
The Diagnostic Challenge: The average time from symptom onset to definitive diagnosis is 2-3 months. Patients often see multiple doctors before mesothelioma is considered, typically after a lack of response to treatments for more common ailments.
Part 4: The Diagnostic Pathway – From Suspicion to Staging
Diagnosis requires a high index of suspicion, especially with a history of asbestos exposure.
Imaging:
Chest X-ray: May show pleural effusion or thickening.
CT Scan of Chest/Abdomen: The primary imaging tool. Reveals pleural thickening, nodules, effusion, and invasion of nearby structures.
PET/CT Scan: Essential for staging. Identifies metabolically active tumor sites and distant metastases.
Biopsy (The Definitive Step): Imaging alone cannot confirm mesothelioma. Tissue is required.
Thoracoscopy (for pleural) or Laparoscopy (for peritoneal): The gold standard. A camera-assisted surgical procedure allows direct visualization and acquisition of large tissue samples, crucial for accurate histologic subtyping.
Less Invasive Biopsies: CT-guided needle biopsies can be used but often yield smaller, less diagnostic samples.
Pathology & Histologic Subtypes: Pathologists use special stains (e.g., calretinin, WT-1) to differentiate mesothelioma from adenocarcinoma. Three main subtypes exist, with prognostic implications:
Epithelioid (60-70%): Best prognosis, more responsive to treatment.
Sarcomatoid (10-20%): Most aggressive, poorest prognosis.
Biphasic/Mixed (10-20%): Contains both epithelioid and sarcomatoid components.
Staging: Uses the TNM system. Most patients present with Stage III or IV disease, where the tumor is locally advanced or has metastasized.
Part 5: The Multimodal Treatment Arsenal – A Focus on Cytoreduction
There is no cure for advanced mesothelioma. Treatment aims to control the disease, alleviate symptoms, and prolong life. Decisions are guided by cell type, stage, and patient fitness.
For Pleural Mesothelioma:
Surgery (For Highly Selected Patients with Early-Stage Epithelioid Disease):
Extrapleural Pneumonectomy (EPP): Radical removal of the lung, pleura, diaphragm, and pericardium. Morbidity is high.
Pleurectomy/Decortication (P/D): More lung-sparing; removes all visible tumor from the pleura and lung surface. Increasingly preferred.
Chemotherapy: The backbone of systemic treatment.
First-Line: Pemetrexed + Cisplatin/Carboplatin. This combination, established in 2003, remains standard, offering a modest survival benefit.
Radiation Therapy: Used palliatively to control pain or bleeding. Rarely used curatively due to the large target area and risk of damaging the lung.
Multimodal Therapy: Combining surgery with chemotherapy (neoadjuvant or adjuvant) and sometimes radiation. Offers the best chance for long-term survival in eligible patients.
For Peritoneal Mesothelioma: A More Promising Approach
Novel and Emerging Therapies:
Immunotherapy: A major breakthrough.
Targeted Therapy: For tumors with specific mutations (e.g., BAP1 loss).
Tumor Treating Fields (TTFields): A wearable device that delivers low-intensity electrical fields to disrupt cancer cell division. Approved for use with chemotherapy in pleural mesothelioma.
Palliative Care:
Integrated early, palliative care is essential to manage symptoms like pain, dyspnea (thoracentesis, pleurodesis), and ascites (paracentesis), and to support quality of life.
Part 6: Prognosis, Legal Recourse, and Prevention
Prognosis: Remains poor overall. Median survival for advanced pleural disease is 12-18 months with chemotherapy, but can be longer with immunotherapy or in selected surgical candidates. Peritoneal disease survival has improved markedly with CRS/HIPEC.
Legal Aspects: In many countries, mesothelioma is a recognized industrial disease. Patients and families have the right to seek compensation from former employers or asbestos trust funds through personal injury or wrongful death lawsuits.
Prevention: Primary prevention is absolute. Over 60 countries have banned asbestos. The ongoing priority is:
Banning all forms of asbestos worldwide.
Safely managing and removing existing asbestos in buildings.
Protecting workers during remediation with strict safety protocols.
Conclusion: A Disease of the Past With a Present-Day Fight
Mesothelioma is a poignant reminder of the long-term consequences of industrial hazards. It is a disease rooted in history but fought with modern oncology’s most sophisticated tools. While the legacy of past exposures will continue to generate new cases for decades, progress is being made. Earlier diagnosis through increased awareness, more effective systemic therapies like immunotherapy, and aggressive regional treatments like HIPEC are slowly changing the trajectory of this devastating cancer. For patients, the journey involves not only medical treatment but also navigating legal and support systems. The ultimate goal remains a future where mesothelioma is not just treatable, but preventable—a relic of a bygone industrial era.
Key Resources for Patients & Families:
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of an oncologist specializing in thoracic or peritoneal malignancies for the management of mesothelioma.