Chemotherapy: A Comprehensive Guide to the Cornerstone of Systemic Cancer Treatment
Introduction: The Double-Edged Sword
Chemotherapy represents one of the most powerful, feared, and misunderstood pillars of modern oncology. Derived from the Greek words for “chemical” and “treatment,” it refers to the use of cytotoxic drugs to destroy cancer cells, primarily by interfering with their ability to divide and multiply. Unlike surgery or radiation, which are local treatments, chemotherapy is a systemic therapy—it travels through the bloodstream to reach cancer cells anywhere in the body. Its legacy is one of profound success, transforming once uniformly fatal cancers like certain leukemias, lymphomas, and testicular cancers into curable diseases. Yet, this power comes at a significant cost: its mechanism of action is not perfectly selective, and it damages rapidly dividing healthy cells alongside cancerous ones, leading to the constellation of side effects for which it is infamous. This guide provides a detailed exploration of chemotherapy’s evolution, mechanisms, clinical application, side effect management, and its evolving role in the era of targeted and immune-based therapies.
Part 1: The Historical Evolution and Modern Context
The birth of modern chemotherapy was serendipitous. During World War II, it was observed that soldiers exposed to nitrogen mustard gas experienced severe depletion of lymphocytes. This led to the first clinical trials in the 1940s using nitrogen mustard analogs to treat lymphoma, marking the beginning of systemic cancer drug therapy.
Since then, chemotherapy has evolved through distinct eras:
1940s-1960s: Discovery of single-agent drugs like methotrexate and 5-fluorouracil.
1970s-1990s: The rise of combination chemotherapy (using multiple drugs with different mechanisms and side effects to increase efficacy and reduce resistance), which dramatically improved cure rates. Adjuvant and neoadjuvant concepts were established.
2000s-Present: Chemotherapy’s role is being refined and redefined. It is increasingly combined with or sequenced alongside more precise targeted therapies and immunotherapies, often serving as a crucial “backbone” to enhance their effects or treat cancers where newer agents are ineffective.
Part 2: The Core Principles: How Chemotherapy Works
Chemotherapy drugs are classified by their mechanism of action and their cell cycle specificity.
Primary Mechanisms of Action:
Alkylating Agents (e.g., Cyclophosphamide, Cisplatin): Directly damage DNA by adding alkyl groups, causing cross-linking and strand breaks that prevent replication.
Antimetabolites (e.g., Methotrexate, 5-FU, Gemcitabine): Mimic essential cellular metabolites (like folic acid or nucleosides), getting incorporated into DNA/RNA during synthesis and halting the process.
Anti-Tumor Antibiotics (e.g., Doxorubicin, Bleomycin): Often derived from soil fungi. They bind to DNA and interfere with the action of topoisomerase enzymes, causing DNA strands to break.
Topoisomerase Inhibitors (e.g., Irinotecan, Etoposide): Specifically target topoisomerase I or II enzymes, crucial for unwinding DNA for replication, leading to fatal DNA breaks.
Mitotic Inhibitors (e.g., Paclitaxel, Vincristine): Disrupt the function of microtubules, the cellular “scaffolding” required for cell division (mitosis), freezing the cell in metaphase.
Corticosteroids (e.g., Dexamethasone, Prednisone): Often used as supportive agents but have direct cytotoxic effects on lymphomas and leukemias.
Cell Cycle Concepts:
Cell Cycle-Specific Drugs: Only work during a specific phase of the cell cycle (e.g., S-phase for antimetabolites, M-phase for mitotic inhibitors). They are most effective against tumors with a high growth fraction.
Cell Cycle-Non-Specific Drugs: Work at any point in the cell cycle, including resting G0 phase (e.g., alkylating agents). They are effective against both slow- and fast-growing tumors.
Part 3: The Goals of Chemotherapy: More Than Just Cure
Chemotherapy is administered with specific therapeutic intent, which dictates the regimen’s intensity and duration.
Curative Intent: To eliminate all cancer cells, resulting in a durable, lifelong remission. Used for many hematologic cancers, testicular cancer, and some solid tumors in early stages (e.g., with adjuvant therapy).
Adjuvant Therapy: Given after primary curative treatment (surgery/radiation) to eradicate microscopic residual disease and reduce the risk of recurrence (e.g., in breast, colon cancer).
Neoadjuvant Therapy: Given before primary local treatment to shrink a tumor, making it easier to remove surgically (downstaging), and to assess tumor response. Common in breast, rectal, and esophageal cancers.
Palliative Intent: For advanced, incurable cancer. The goal is to control tumor growth, alleviate symptoms (e.g., pain, obstruction), improve quality of life, and prolong survival without expectation of cure.
Myeloablative Therapy: Ultra-high dose chemotherapy used to completely ablate the bone marrow immediately prior to a stem cell or bone marrow transplant.
Part 4: Administration and Treatment Planning
Chemotherapy is not a single event but a carefully planned cycle of treatment and recovery.
Routes of Administration:
Intravenous (IV): Most common, allows for controlled infusion.
Oral: Increasingly available (e.g., capecitabine, temozolomide).
Intramuscular, Subcutaneous, Intrathecal (into spinal fluid), Intraperitoneal (into abdominal cavity), Topical.
Treatment Cycles: Chemotherapy is given in cycles (e.g., every 2 or 3 weeks) to allow normal cells, especially in the bone marrow, time to recover between treatments. A course of treatment comprises multiple cycles.
Dose Calculation: Doses are meticulously calculated based on body surface area (BSA) or weight to maximize efficacy while minimizing toxicity.
The Multidisciplinary Team: Decisions are made by a medical oncologist in collaboration with pharmacists, specialized nurses, and supportive care teams.
Part 5: Managing Side Effects – The Art of Supportive Care
Proactive management of side effects is a critical component of modern chemotherapy, allowing patients to complete planned treatment and maintain quality of life.
Common Side Effects and Management Strategies:
Myelosuppression (Low Blood Counts): The most common dose-limiting toxicity.
Neutropenia (low white cells): Risk of life-threatening infection. Managed with growth factor injections (G-CSF) and prophylactic antibiotics.
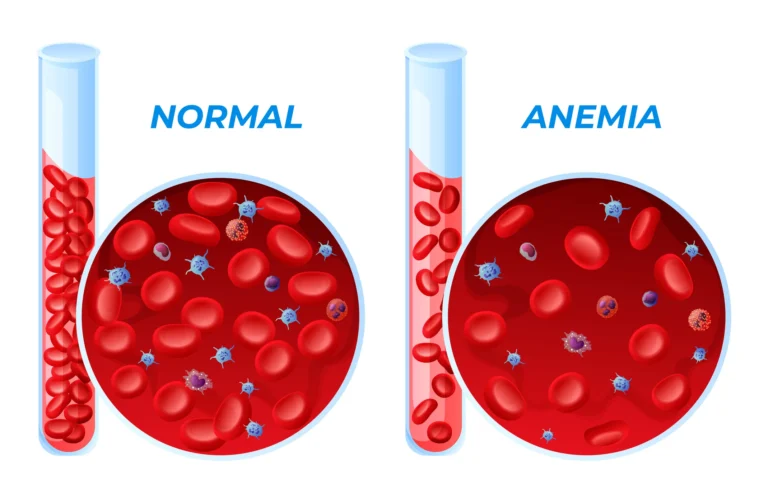
Anemia (low red cells): Causes fatigue. Treated with iron, erythropoiesis-stimulating agents (ESAs), or blood transfusions.
Thrombocytopenia (low platelets): Risk of bleeding. Managed with platelet transfusions.
Nausea and Vomiting: Classified as acute, delayed, or anticipatory. Highly preventable with modern antiemetic regimens using 5-HT3 antagonists (ondansetron), NK1 antagonists (aprepitant), and dexamethasone.
Fatigue: Multifactorial. Managed with energy conservation, gentle exercise, and treating contributing factors (anemia, poor sleep).
Alopecia (Hair Loss): Caused by damage to hair follicle cells. Scalp cooling caps (cold capping) can reduce hair loss for some regimens.
Mucositis (Mouth Sores): Painful inflammation of the digestive tract lining. Managed with good oral hygiene, cryotherapy (ice chips), and pain medications.
Peripheral Neuropathy: Numbness, tingling, or pain in hands/feet from nerve damage (common with taxanes, platinums). Dose adjustments, supplements (like alpha-lipoic acid), and medications (gabapentin) are used.
“Chemo Brain”: Cognitive changes like memory lapses and foggy thinking. Managed with cognitive rehabilitation, planners, and rest.
Long-Term & Late Effects: Including infertility, cardiac toxicity (from anthracyclines), secondary cancers, and permanent organ damage (kidneys, lungs, nerves). Pre-treatment counseling and long-term survivorship plans are essential.
Part 6: Chemotherapy in the Modern Era: Combination and Precision
Chemotherapy is rarely used in isolation today. Its role is integrated into a broader therapeutic strategy:
Combination with Targeted Therapy: e.g., Trastuzumab + chemo for HER2+ breast cancer; Bevacizumab + chemo for colorectal cancer.
Combination with Immunotherapy: e.g., Pembrolizumab + chemo as first-line for many lung cancers; chemo may help expose cancer cells to the immune system.
Dose-Dense Chemotherapy: Administering cycles more frequently (with growth factor support) to overcome rapid tumor regrowth.
Metronomic Chemotherapy: Low-dose, continuous oral administration to target tumor blood vessels and modulate the immune environment with fewer side effects.
The Future: Research focuses on nanoparticle delivery systems to target drugs more specifically to tumors, reducing systemic exposure, and developing biomarkers to predict which patients will benefit from or be resistant to specific chemotherapies.
Conclusion: An Enduring Pillar, Evolving in Purpose
Chemotherapy remains a cornerstone of cancer treatment, responsible for millions of cures and years of life extended. Its narrative has shifted from one of unmitigated toxicity to one of strategic power within a precision oncology framework. While the quest for more selective, less toxic treatments continues, chemotherapy’s unique ability to kill rapidly dividing cells en masse ensures its enduring relevance. For patients, understanding its mechanisms, goals, and the robust supportive care available can transform the experience from one of dread to one of informed partnership in a challenging but potentially life-saving treatment journey.
Key Takeaways for Patients:
Chemotherapy is a systemic treatment with specific, often curative, goals.
Not all regimens cause the same side effects. Discuss the expected toxicities of your specific drugs.
Modern supportive care is highly effective at preventing and managing nausea, low blood counts, and other side effects.
Discuss fertility preservation, cardiac risk, and other long-term effects with your oncologist before starting treatment.
Chemotherapy is increasingly used in rational combination with newer, more targeted drugs.
Resources:
American Cancer Society: “A Guide to Chemotherapy”
National Cancer Institute: Chemotherapy side effect management.
CancerCare: Free professional support services.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. All decisions regarding chemotherapy must be made in close consultation with a qualified medical oncologist.