Cervical Cancer: A Comprehensive Guide to the Preventable and Curable Cancer
Introduction: A Paradigm of Prevention in Oncology
Cervical cancer occupies a unique and hopeful space in the world of oncology. It is a cancer that is both highly preventable and, when detected early, highly curable. Yet, it remains a leading cause of cancer death for women in regions with limited access to healthcare, starkly highlighting the global inequity in cancer outcomes. Virtually all cases (over 95%) are caused by persistent infection with high-risk strains of the Human Papillomavirus (HPV), a common sexually transmitted infection. This clear etiological agent has allowed for the development of two powerful shields: HPV vaccination for primary prevention and cervical screening (Pap/HPV tests) for secondary prevention. The slow progression from HPV infection to pre-cancer to invasive cancer—taking 10 to 20 years—provides a critical window for intervention. This guide details the journey from HPV infection to cancer, the pivotal role of prevention, and the modern management of cervical cancer.
Part 1: The Biology: From HPV Infection to Invasive Cancer
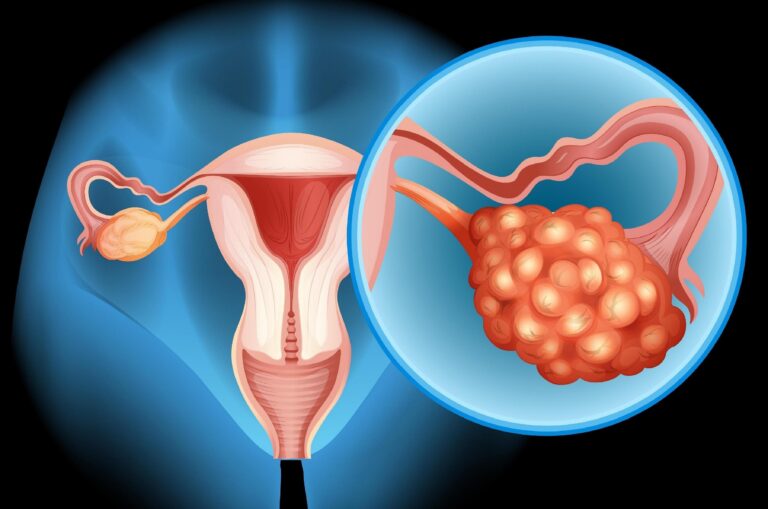
The cervix is the lower, narrow part of the uterus that connects to the vagina. Cervical cancer arises in the transformation zone, where the glandular cells of the endocervix meet the squamous cells of the ectocervix.
The Carcinogenic Cascade:
HPV Infection: Infection with a high-risk HPV type (most commonly HPV 16 and 18, which cause ~70% of cases) is sexually acquired. Most infections are cleared by the immune system within 1-2 years.
Persistent Infection: In a small percentage of women, the infection persists. Viral DNA integrates into the host cell’s genome, leading to the production of viral oncoproteins E6 and E7. These proteins inactivate crucial tumor suppressor proteins (p53 and Rb), disrupting the cell cycle and allowing uncontrolled growth.
Pre-Cancerous Changes (Cervical Intraepithelial Neoplasia – CIN):
CIN 1 (Low-Grade): Mild dysplasia; often regresses spontaneously.
CIN 2/3 (High-Grade): Moderate to severe dysplasia; considered a direct precursor to invasive cancer. These lesions are detectable and treatable years before cancer develops.
Invasive Cervical Cancer: Cancer cells break through the basement membrane of the epithelium and invade the cervical stroma, gaining the potential to spread (metastasize).
Part 2: Risk Factors and the Power of Prevention
Primary Risk Factor:
Co-Factors That Increase Risk Given an HPV Infection:
Smoking: Doubles the risk. Toxins concentrate in cervical mucus, damaging DNA and impairing local immune response.
Immunosuppression: HIV infection or immunosuppressive medications (e.g., after organ transplant) greatly increase the risk of persistence and progression.
Long-Term Use of Oral Contraceptives (≥5 years).
High Parity (multiple full-term pregnancies).
Co-infection with other sexually transmitted infections (e.g., chlamydia, herpes).
Socioeconomic Factors: Limited access to screening and vaccination.
The Two Pillars of Prevention:
Primary Prevention: HPV Vaccination
Vaccines: Gardasil 9 protects against 9 HPV types (6, 11, 16, 18, 31, 33, 45, 52, 58).
Recommendation: For all adolescents (boys and girls) aged 11-12, but can be given as early as age 9 and up to age 45. It is most effective when given before sexual debut.
Impact: Countries with high vaccination coverage have seen dramatic declines in HPV infections, genital warts, and pre-cancerous lesions.
Secondary Prevention: Cervical Screening
Pap Test (Pap Smear): Collects cervical cells to look for abnormal cytology.
HPV Test: Detects the presence of high-risk HPV DNA.
Co-testing: Both tests performed together (preferred for ages 30-65).
Screening Guidelines (U.S.):
Ages 21-29: Pap test every 3 years.
Ages 30-65: Co-testing every 5 years (preferred) or Pap test every 3 years.
Over 65: May stop if prior adequate screening is negative.
Action for Abnormal Results: May lead to colposcopy (magnified exam of the cervix) with biopsy, and treatment of pre-cancer (e.g., LEEP, cryotherapy), which prevents cancer from developing.
Part 3: Signs, Symptoms, and the Critical Importance of Early Detection
Pre-cancer and early-stage cervical cancer often have NO symptoms. This is why regular screening is non-negotiable.
Symptoms of Invasive Cancer (When They Occur):
Abnormal Vaginal Bleeding: The most common symptom.
Bleeding after intercourse (postcoital bleeding).
Bleeding between menstrual periods.
Heavier or longer menstrual periods.
Any vaginal bleeding after menopause.
Unusual Vaginal Discharge: May be watery, pink, foul-smelling, or heavy.
Pelvic Pain or Pain During Intercourse.
Any of these symptoms warrant immediate evaluation by a gynecologist. Do not assume bleeding is from hemorrhoids or irregular cycles.
Part 4: Diagnosis and Staging – Determining the Extent of Disease
If screening or symptoms suggest cancer, a diagnostic workup is performed.
Colposcopy & Biopsy: The cornerstone of diagnosis. A special microscope (colposcope) examines the cervix. Abnormal areas are biopsied. A cone biopsy (conization) may be needed to diagnose early invasion.
Pathology: Confirms the diagnosis and histological type:
Squamous Cell Carcinoma (~80%): Arises from squamous cells.
Adenocarcinoma (~20%): Arises from glandular cells. Often harder to detect by Pap smear.
Other rare types: Adenosquamous, neuroendocrine.
Staging: Cervical cancer is clinically staged (based on physical exam, imaging, and limited procedures), not surgically staged. The FIGO (International Federation of Gynecology and Obstetrics) system is used.
Stage I: Confined to the cervix.
Stage II: Invades beyond uterus but not to pelvic wall or lower third of vagina.
Stage III: Extends to pelvic wall, lower vagina, or causes kidney problems.
Stage IV: Invades bladder/rectum or has distant metastases.
Imaging: Pelvic MRI is best for evaluating local tumor extent. CT scan of chest/abdomen/pelvis or PET/CT is used to check for lymph node involvement and distant metastases.
Part 5: Treatment – A Stage-Dependent, Multimodal Approach
Treatment is determined by FIGO stage, tumor size, histology, desire for fertility, and patient health. A multidisciplinary team is essential.
For Early-Stage Disease (Stage IA1 – IB2):
Fertility-Sparing Surgery: For select small tumors in women wishing to preserve fertility.
Standard Surgery: Radical Hysterectomy (removal of uterus, cervix, parametrium, upper vagina) with Pelvic Lymph Node Dissection. Often performed with minimally invasive techniques.
For Locally Advanced Disease (Stage IB3 – IVA):
Primary Chemoradiation (Concurrent Chemoradiotherapy – CCRT): The global standard of care.
External Beam Radiation Therapy (EBRT): Targets the primary tumor and pelvic lymph nodes.
Brachytherapy: The crucial component. A radioactive source is placed inside the vagina/uterus, delivering a high dose directly to the cervix.
Concurrent Chemotherapy: Typically weekly Cisplatin, a radiosensitizer that enhances the effect of radiation.
Role of Surgery: Sometimes performed after chemoradiation (adjuvant hysterectomy) in specific high-risk situations, but not routinely.
For Metastatic/Recurrent Disease (Stage IVB):
Systemic Therapy: The primary approach.
Chemotherapy: Combinations like carboplatin/paclitaxel with bevacizumab (an anti-angiogenic drug) are standard first-line, improving survival.
Immunotherapy: Pembrolizumab is approved for recurrent/metastatic cervical cancer that is PD-L1 positive, often combined with chemotherapy ± bevacizumab.
Targeted Therapy: Tisotumab vedotin, an antibody-drug conjugate, is approved for recurrent/metastatic disease.
Palliative Radiation: To control pain, bleeding, or other symptoms from metastases.
Part 6: Prognosis, Survivorship, and Global Disparities
Prognosis: Is excellent when detected early. The 5-year survival rate for localized cervical cancer is over 90%. It drops significantly for regional (58%) and distant (17%) stages, highlighting the life-saving importance of screening and early treatment.
Survivorship: Involves monitoring for recurrence, managing long-term side effects of treatment (lymphedema, early menopause, vaginal stenosis, bladder/bowel issues), and providing psychosocial support.
The Global Challenge: Over 90% of cervical cancer deaths occur in low- and middle-income countries. The WHO has launched a global strategy to eliminate cervical cancer through: 90% HPV vaccination coverage, 70% screening coverage, and 90% treatment of pre-cancer/invasive disease by 2030.
Conclusion: A Path to Elimination
Cervical cancer stands as a testament to what is possible in cancer control. It is a disease with a known cause, effective prevention tools, and curative treatments for early-stage disease. The path forward is clear: universal HPV vaccination, equitable access to high-quality screening, and timely treatment. For individuals, this means getting vaccinated, adhering to screening guidelines, and seeking prompt medical attention for any symptoms. For the global community, it means committing to closing the equity gap. Through these concerted efforts, cervical cancer can and should be relegated to the history books, becoming a rare disease rather than a global killer.
Key Takeaways & Call to Action:
Get your children (sons and daughters) vaccinated against HPV.
Adhere to recommended cervical screening guidelines—it can catch pre-cancer before it turns into cancer.
Never ignore abnormal vaginal bleeding—see your doctor immediately.
Support global efforts to make vaccination, screening, and treatment accessible to all women, everywhere.
Resources:
American Cancer Society: www.cancer.org
National Cervical Cancer Coalition: www.nccc-online.org
World Health Organization (WHO): Global strategy to eliminate cervical cancer.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your gynecologist or oncologist with any questions you may have regarding your health.