Heartburn: A Comprehensive Guide to the Burning Reality of Gastroesophageal Reflux
Introduction: More Than Just a Discomfort
Heartburn, that familiar, uncomfortable burning sensation rising from the stomach into the chest and throat, is one of the most common gastrointestinal complaints worldwide. While often dismissed as a minor nuisance after a spicy meal, frequent heartburn is the cardinal symptom of Gastroesophageal Reflux Disease (GERD), a chronic, progressive condition with far-reaching implications. It occurs when the sophisticated barrier between the stomach and esophagus fails, allowing acidic or non-acidic stomach contents to “reflux” upward. Understanding heartburn is not just about finding quick relief; it’s about recognizing when a simple symptom signals a deeper dysfunction that can lead to complications like esophagitis, strictures, Barrett’s esophagus, and even esophageal cancer. This guide details the mechanics of reflux, the spectrum of symptoms, evidence-based management, and the critical line between self-care and medical intervention.
Part 1: The Anatomy of Reflux – A Flawed Valve
To understand heartburn, one must understand the lower esophageal sphincter (LES) and the diaphragm.
The Lower Esophageal Sphincter (LES): A ring of specialized muscle at the junction of the esophagus and stomach. It functions as a one-way valve, tightening to prevent stomach contents from flowing backward.
The Diaphragmatic Crura: The LES is anchored by the diaphragm’s muscle fibers. This partnership is essential for creating adequate pressure to keep the valve closed.
The Breakdown (The Pathophysiology of Reflux):
Transient LES Relaxations (TLESRs): The most common cause. The LES inappropriately relaxes for periods unrelated to swallowing, allowing gastric contents to reflux.
Hypotensive LES: A chronically weak LES with insufficient resting pressure.
Anatomic Disruption: A hiatal hernia, where part of the stomach protrudes through the diaphragm into the chest, physically disrupts the LES-diaphragm partnership, severely compromising the anti-reflux barrier.
The Irritant: Refluxed material can be acidic (hydrochloric acid, pepsin) or non-acidic (bile, pancreatic enzymes). Both can cause symptoms and tissue damage.
Part 2: Symptoms – Beyond the Classic Burn
While retrosternal burning is classic, GERD is a master of mimicry, presenting with an array of typical and atypical symptoms.
Typical (Esophageal) Symptoms:
Heartburn (Pyrosis): A burning sensation rising from the upper abdomen or lower chest toward the neck. Often worse after meals, when lying down, or bending over.
Regurgitation: The effortless return of bitter or sour-tasting fluid or undigested food into the throat or mouth. A feeling of “wet burps.”
Dysphagia: Difficulty swallowing. Can indicate inflammation, a stricture (narrowing), or malignancy.
Odynophagia: Painful swallowing (suggests severe esophagitis).
Atypical (Extra-esophageal) Symptoms:
These occur when refluxate reaches beyond the esophagus, causing inflammation in adjacent structures.
Chronic Cough: A persistent, dry cough, often worse at night or after meals. A leading cause of unexplained chronic cough.
Laryngopharyngeal Reflux (LPR) / “Silent Reflux”: Hoarseness, chronic throat clearing, sensation of a lump in the throat (globus), post-nasal drip, sore throat. Often lacks classic heartburn.
Asthma & Wheezing: Reflux can trigger bronchoconstriction or microaspiration, worsening asthma, especially nocturnal asthma.
Dental Erosion: Acid wearing away tooth enamel.
Non-Cardiac Chest Pain: Can be severe and mimic angina or a heart attack. Any new or unexplained chest pain requires immediate evaluation to rule out cardiac causes first.
Alarm Symptoms (Require Prompt Medical Evaluation):
Difficulty or pain with swallowing (dysphagia/odynophagia).
Unintentional weight loss.
Gastrointestinal bleeding (vomiting blood or coffee-ground material, black/tarry stools).
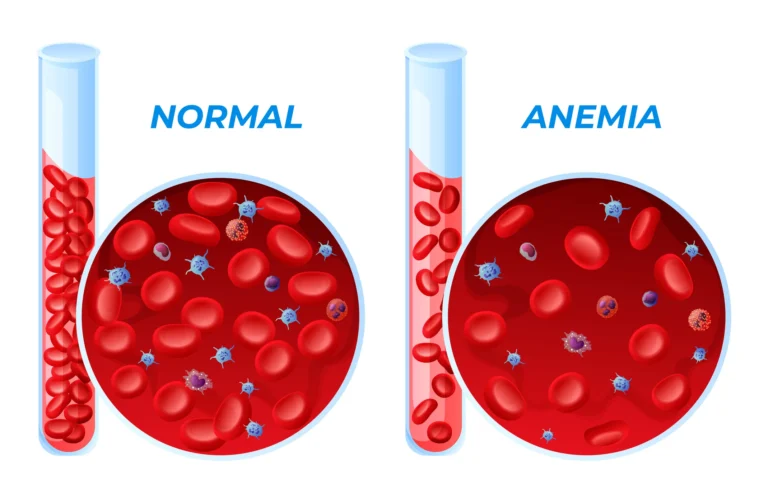
Anemia.
Symptoms starting after age 50.
Persistent symptoms despite adequate PPI therapy.
Part 3: Triggers and Risk Factors – Lifestyle and Biology
Reflux results from a combination of factors that increase abdominal pressure, weaken the LES, or directly irritate the esophagus.
Lifestyle & Dietary Triggers:
Foods: Chocolate, caffeine, peppermint, fatty/fried foods, spicy foods, citrus, tomatoes, onions, garlic.
Beverages: Alcohol, carbonated drinks, acidic juices.
Habits: Large meals, eating within 2-3 hours of bedtime, smoking (relaxes LES, reduces saliva).
Medications: Calcium channel blockers, nitrates, some asthma meds, anticholinergics, bisphosphonates.
Biological & Structural Risk Factors:
Hiatal Hernia: A major anatomical risk factor.
Obesity: Increased abdominal pressure forces stomach contents upward.
Pregnancy: Hormonal changes relax the LES; the growing uterus increases intra-abdominal pressure.
Delayed Gastric Emptying: Food sits in the stomach longer, increasing reflux opportunity.
Connective Tissue Disorders (e.g., scleroderma).
Part 4: Diagnosis – Is It Just Heartburn?
For typical heartburn responsive to lifestyle changes or OTC meds, formal testing may not be needed. Investigation is warranted for alarm symptoms, atypical presentations, or inadequate response to treatment.
Empirical PPI Trial: A therapeutic trial of a high-dose proton pump inhibitor (PPI) for 4-8 weeks. Symptom improvement supports a GERD diagnosis.
Upper Endoscopy (EGD): The primary diagnostic tool. A camera examines the esophagus, stomach, and duodenum. It can diagnose:
Ambulatory Reflux Monitoring: The gold standard for objective diagnosis. A thin catheter or wireless capsule measures acid/non-acid reflux events in the esophagus over 24-96 hours. Crucial when endoscopy is normal but symptoms persist.
Esophageal Manometry: Measures the pressure and coordination of esophageal contractions and LES function. Used prior to anti-reflux surgery.
Part 5: Management – A Stepwise, Long-Term Strategy
Management aims to control symptoms, heal esophagitis, and prevent complications. It is often lifelong.
Step 1: Lifestyle and Dietary Modifications (Foundation for All):
Weight loss if overweight.
Elevate the head of the bed 6-8 inches (using blocks, not just pillows).
Avoid eating within 3 hours of bedtime.
Identify and eliminate personal dietary triggers.
Stop smoking and limit alcohol.
Wear loose-fitting clothing.
Step 2: Pharmacologic Therapy (Step-Up or Step-Down Approach):
Antacids (e.g., Tums, Mylanta): Provide rapid, short-term neutralization of acid. Good for occasional heartburn.
H2-Receptor Antagonists (H2RAs: e.g., Famotidine/Pepcid, Ranitidine): Reduce acid production for 6-12 hours. Can lose efficacy over time (tachyphylaxis).
Proton Pump Inhibitors (PPIs: e.g., Omeprazole, Esomeprazole, Pantoprazole): The most effective medical therapy. They irreversibly block the stomach’s acid pump, providing profound and sustained acid suppression. Used for healing esophagitis and long-term symptom control.
Critical Considerations: Should be taken 30-60 minutes before the first meal of the day. Long-term use requires awareness of potential (but often overstated) risks (B12 deficiency, osteoporosis risk, kidney disease, C. diff infection). The benefit of preventing esophageal damage usually outweighs these risks. Do not stop abruptly (risk of rebound hyperacidity).
Step 3: Procedural and Surgical Interventions:
For patients with refractory symptoms, intolerance to medications, or desire to discontinue lifelong drugs.
Transoral Incisionless Fundoplication (TIF): An endoscopic procedure that reconstructs the anti-reflux valve.
Magnetic Sphincter Augmentation (LINX Device): A ring of magnetic beads surgically placed around the LES, reinforcing it while allowing food to pass.
Laparoscopic Nissen Fundoplication: The traditional gold-standard surgery. The top of the stomach is wrapped around the LES to strengthen it. Highly effective but carries risks of bloating and dysphagia.
Part 6: Complications of Chronic, Untreated GERD
Persistent acid exposure damages the esophageal lining, leading to:
Erosive Esophagitis: Inflammation, ulcers, and bleeding.
Esophageal Stricture: Scarring and narrowing causing progressive dysphagia.
Barrett’s Esophagus: The most significant complication. The body attempts to heal by replacing squamous cells with acid-resistant columnar cells. This metaplastic change increases the risk of esophageal adenocarcinoma by 30-125 times. Requires regular surveillance endoscopy with biopsies.
Esophageal Adenocarcinoma: A cancer with a rapidly rising incidence in the West, strongly linked to chronic GERD and Barrett’s.
Conclusion: Respecting the Burn
Heartburn is a signal, not just a sensation. While manageable for most, it demands respect as the tip of the GERD iceberg. Effective management requires a partnership between patient and physician, blending disciplined lifestyle changes with appropriate, monitored medication use. Recognizing alarm symptoms and understanding the potential for serious complications like Barrett’s esophagus are crucial. By moving beyond temporary relief to a strategic, long-term management plan, individuals can effectively control symptoms, protect their esophageal health, and maintain a high quality of life.
Key Takeaways:
Frequent heartburn (2+ times/week) is GERD, not normal.
Never ignore alarm symptoms like trouble swallowing or weight loss.
Lifestyle changes are the foundation, but PPIs are the most effective medical therapy for chronic cases.
Long-term PPI use should be at the lowest effective dose, guided by a doctor, not feared.
Chronic GERD requires monitoring for complications like Barrett’s esophagus.
When to See a Doctor:
Heartburn occurring more than twice a week.
Symptoms persist despite over-the-counter medications.
You experience any alarm symptom.
You’ve needed to use OTC heartburn meds for more than two weeks.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your gastroenterologist or primary care physician with any questions regarding a medical condition.