Male Infertility: A Comprehensive Guide to Causes, Diagnosis, and Modern Treatment
Introduction: Shattering the Silence and Stigma
Male infertility is a common, yet often unspoken, medical condition affecting approximately 1 in 3 couples struggling to conceive. It is defined as the inability of a male to achieve a pregnancy in a fertile female partner after at least one year of regular, unprotected intercourse. For decades, the burden of infertility was disproportionately and erroneously placed on women, but modern andrology has revealed that a male factor is the sole or contributing cause in roughly 50% of cases. Male infertility is not a monolithic condition; it is a symptom of an underlying biological disruption in the complex process of sperm production, maturation, or delivery. Moving beyond stigma and misconception is the first step toward effective diagnosis and treatment, empowering men to become active, informed partners in their reproductive journey.
Part 1: The Physiology of Fertility – How Sperm Production Works
Understanding infertility requires a basic grasp of normal male reproductive physiology.
The Hypothalamic-Pituitary-Gonadal (HPG) Axis: The brain’s command center. The hypothalamus releases GnRH, stimulating the pituitary gland to secrete Follicle-Stimulating Hormone (FSH) and Luteinizing Hormone (LH).
LH signals the Leydig cells in the testes to produce testosterone.
FSH (with testosterone) acts on Sertoli cells to support spermatogenesis—the 72-day process of sperm creation within the seminiferous tubules.
Sperm Maturation & Transport: Immature sperm travel from the testes to the epididymis for maturation and storage. During ejaculation, they mix with fluids from the seminal vesicles and prostate gland to form semen, which is expelled via the vas deferens and urethra.
A disruption at any point in this axis or pathway can lead to infertility.
Part 2: Causes of Male Infertility – A Multifactorial Problem
Causes are typically categorized by where the problem occurs.
1. Pre-testicular Causes (Hormonal/Endocrine):
Problems with the brain’s signaling system.
Hypogonadotropic Hypogonadism: Low FSH/LH due to pituitary tumors (e.g., prolactinoma), Kallmann syndrome, anabolic steroid abuse, or extreme stress/illness.
Hyperprolactinemia: Elevated prolactin suppresses GnRH.
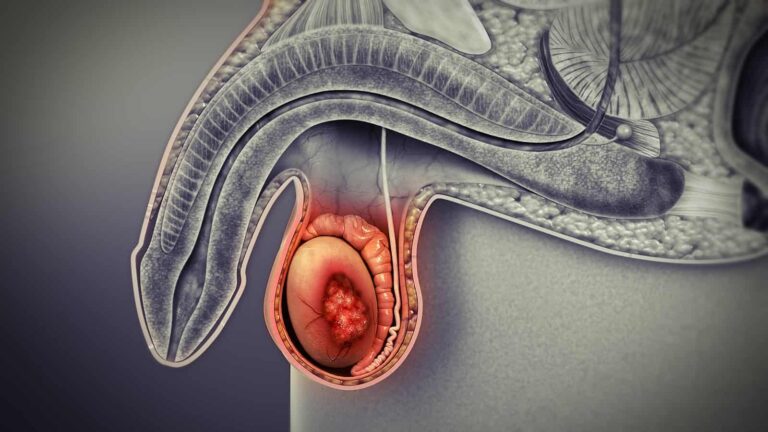
2. Testicular Causes (Primary Gonadal Failure):
Direct damage to the sperm factories.
Genetic Disorders:
Klinefelter Syndrome (XXY): The most common genetic cause. Leads to small, firm testes and azoospermia (no sperm in semen).
Y-Chromosome Microdeletions: Missing genetic material critical for sperm production.
Cryptorchidism: Undescended testes, even if surgically corrected, can impair sperm production.
Varicocele: The most common correctable cause (~40% of cases). Dilated veins in the scrotum increase testicular temperature, impairing spermatogenesis.
Infection/Inflammation (Orchitis): Mumps, sexually transmitted infections.
Trauma or Torsion.
Cancer Treatments: Chemotherapy and radiation are toxic to germ cells.
Environmental Toxins & Lifestyle: Prolonged heat exposure (hot tubs, laptops), pesticides, heavy metals, smoking, excessive alcohol, and obesity.
3. Post-testicular Causes (Obstructive):
Sperm are produced but cannot be ejaculated.
Obstruction of the Vas Deferens/Epididymis: From infection (e.g., chlamydia), prior surgery (e.g., hernia repair), or Congenital Bilateral Absence of the Vas Deferens (CBAVD), often associated with cystic fibrosis gene mutations.
Ejaculatory Duct Obstruction.
Retrograde Ejaculation: Semen flows backward into the bladder due to nerve damage from diabetes, spinal cord injury, or prostate/bladder surgery.
Erectile Dysfunction or Anorgasmia.
4. Idiopathic Infertility:
No identifiable cause is found in about 30-40% of cases, often labeled as “unexplained” male infertility, likely due to subtle genetic or molecular defects.
Part 3: The Diagnostic Evaluation – A Systematic Workup
A thorough evaluation by a urologist or reproductive endocrinologist specializing in male infertility (an andrologist) is essential.
Step 1: Comprehensive History & Physical Exam
History: Medical/surgical history, sexual history, duration of infertility, exposures, family history.
Physical Exam: Focus on testicular size/consistency, presence of a varicocele (palpable as a “bag of worms”), vas deferens, and secondary sexual characteristics.
Step 2: Semen Analysis – The Cornerstone Test
At least two samples are analyzed, following WHO guidelines. Key parameters:
Volume: Normal ≥1.5 mL.
Sperm Concentration (Count): Normal ≥15 million sperm/mL.
Total Motility: Normal ≥40% moving.
Progressive Motility: Normal ≥32% moving purposefully forward.
Morphology (Shape): Normal ≥4% have ideal form (strict Kruger criteria).
Additional Tests: Vitality (live vs. dead), presence of white blood cells (indicating infection), and sperm DNA fragmentation (a test for internal genetic damage).
Step 3: Hormonal Profile (Blood Tests)
Testosterone, FSH, LH: To differentiate pre-testicular from testicular causes.
Prolactin, Thyroid (TSH).
Step 4: Advanced Diagnostics (As Indicated)
Scrotal Ultrasound: Visualizes testicular architecture and confirms/assesses varicoceles.
Transrectal Ultrasound (TRUS): Checks for ejaculatory duct obstruction or seminal vesicle anomalies.
Post-Ejaculatory Urinalysis: Diagnoses retrograde ejaculation.
Genetic Testing:
Karyotype: Rules out Klinefelter syndrome.
Y-Chromosome Microdeletion Analysis.
Cystic Fibrosis (CFTR) Gene Mutation Testing: For men with CBAVD or obstructive azoospermia.
Testicular Sperm Extraction (TESE) or Biopsy: For azoospermic men to determine if sperm production is occurring (non-obstructive vs. obstructive).
Part 4: Treatment Strategies – From Lifestyle to Laboratory
Treatment is tailored to the specific cause.
A. Lifestyle & Medical Management:
Lifestyle Modifications: Smoking cessation, reducing alcohol, avoiding heat exposure, weight loss, antioxidant-rich diet (vitamins C, E, coenzyme Q10).
Varicocele Repair (Varicocelectomy): Surgical ligation or embolization of the dilated veins. Can improve semen parameters and natural pregnancy rates.
Hormone Therapy: For hypogonadotropic hypogonadism (e.g., hCG, FSH injections, clomiphene citrate).
Antibiotics: For treatable infections.
Medications for Ejaculatory Dysfunction: Alpha-agonists for retrograde ejaculation.
B. Assisted Reproductive Technology (ART) – The Modern Solution
When natural conception is not possible, ART provides powerful options.
Intrauterine Insemination (IUI):
For: Mild male factor (moderately low count/motility).
Process: Washed, concentrated sperm is placed directly into the uterus around ovulation.
In Vitro Fertilization (IVF):
For: Moderate to severe male factor, unexplained infertility.
Process: Eggs are retrieved from the female partner and fertilized with sperm in a laboratory dish.
Intracytoplasmic Sperm Injection (ICSI) – The Game-Changer:
For: Severe male factor (very low count, poor motility, high DNA fragmentation, obstructive/non-obstructive azoospermia).
Process: A single sperm is injected directly into a single egg under a microscope. ICSI has made fatherhood possible for men who would have been considered sterile a generation ago.
Combined with Sperm Retrieval Techniques: For obstructive azoospermia, sperm can be retrieved via:
C. Addressing Severe Non-Obstructive Azoospermia (NOA):
When no sperm are found in the testes (Sertoli Cell Only Syndrome), options include:
Part 5: Psychological Impact and the Importance of Support
The diagnosis of male infertility can be a profound psychological blow, linked to feelings of shame, inadequacy, depression, and anxiety. It can strain relationships and affect sexual intimacy.
Open Communication between partners is critical.
Professional Counseling with a therapist specializing in infertility can be invaluable.
Support Groups help men realize they are not alone.
Conclusion: A Path Forward Through Science and Partnership
Male infertility is a complex medical condition, not a reflection of masculinity or virility. The field has moved from one of diagnostic ignorance and therapeutic nihilism to one of precise evaluation and highly effective treatments. The journey begins with breaking the silence, seeking expert evaluation, and understanding that a diagnosis is a starting point, not an endpoint. Through a combination of lifestyle changes, medical/surgical interventions, and advanced assisted reproductive technologies like ICSI, the vast majority of men with infertility can achieve their dream of biological fatherhood. By approaching it as a shared medical challenge within a partnership, couples can navigate this path with resilience, hope, and the support of modern reproductive science.
Key Takeaways for Men:
You are not alone; male factors are involved in half of infertility cases.
Seek evaluation early (after 12 months, or 6 months if the female partner is over 35).
The basic workup (history, exam, semen analysis) is straightforward and non-invasive.
Even with severe diagnoses like azoospermia, biological fatherhood is often possible through sperm retrieval and ICSI.
Address the emotional aspect as seriously as the medical one.
Resources:
American Society for Reproductive Medicine (ASRM): Patient resources on male infertility.
Urology Care Foundation: Information on male reproduction.
Resolve: The National Infertility Association: www.resolve.org (Provides support groups and education).
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a urologist or reproductive endocrinologist with any questions regarding male fertility.