Scrotal Pain: A Comprehensive Guide to Diagnosis, Emergencies, and Management
Introduction: The Critical Imperative of Scrotal Pain
Scrotal pain is one of the most compelling and time-sensitive symptoms in men’s health. The scrotum, a protective sac housing the testicles, epididymis, and spermatic cord, is a region of exquisite sensitivity and vital function. Pain here demands immediate and careful evaluation because the differential diagnosis spans from benign, self-limited conditions to true surgical emergencies where delay can lead to permanent organ loss or systemic illness. Unlike pain in other areas where “wait and see” may be an option, scrotal pain operates on a different timeline. Understanding the potential causes and their “red flag” symptoms is not just about comfort—it is about organ preservation.
This detailed guide provides a systematic approach to understanding scrotal pain, categorizing conditions by urgency, outlining diagnostic pathways, and emphasizing the critical decisions that must be made to protect testicular function and overall health.
Part 1: Anatomy and the Nature of Scrotal Pain
To understand the pain, one must understand the structures involved:
Testis (Testicle): The male gonad, responsible for sperm and testosterone production. Has a rich blood supply via the spermatic cord.
Epididymis: A coiled tube capping the rear of the testis, where sperm mature and are stored.
Spermatic Cord: Contains the testicular artery (bringing blood in), pampiniform plexus (veins carrying blood out), and the vas deferens (carrying sperm). This cord suspends the testicle in the scrotum.
Tunica Vaginalis: A two-layered membrane surrounding the testis, which can fill with fluid.
Pain Characteristics: Pain can be acute (sudden onset) or chronic (lasting >3 months). It can be localized to one structure (e.g., the epididymis) or diffuse. Referred pain from the abdomen, kidneys, or groin can also be perceived in the scrotum, complicating diagnosis.
Part 2: The Surgical Emergencies – Conditions Requiring Immediate Intervention
These diagnoses are measured in hours. A delay in treatment can result in testicular infarction (death) and loss of the testicle.
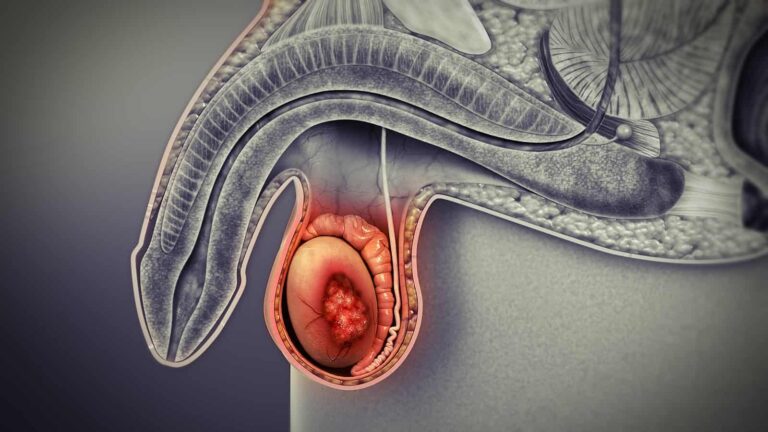
1. Testicular Torsion
What it is: The spermatic cord twists, cutting off the testicle’s blood supply. It is most common in adolescents (peak: 12-18 years) but can occur at any age.
Symptoms:
Sudden, severe, unilateral testicular pain, often waking a patient from sleep.
Pain is often not relieved by lifting the testicle (negative Prehn’s sign).
Testicle may appear high-riding and have a horizontal (“bell-clapper”) orientation.
Nausea and vomiting are common.
Absent or decreased cremasteric reflex (gentle stroking of the inner thigh does not cause the testicle to retract).
Action: A TRUE UROLOGIC EMERGENCY. Diagnosis is clinical, often confirmed by Doppler ultrasound showing absent blood flow. Requires immediate surgical exploration and detorsion (untwisting). If treated within 6 hours, salvage rate is >90%; after 12 hours, it drops drastically.
2. Torsion of a Testicular Appendage
What it is: Twisting of a small, vestigial remnant (like the appendix testis) attached to the testicle or epididymis. Common in boys aged 7-14.
Symptoms: Similar acute onset of pain, but often less severe than full torsion. A small, tender, blue-dotted nodule may be palpable at the upper pole of the testis (“blue dot sign”).
Action: Often managed conservatively with rest, NSAIDs, and scrotal support, as it is self-limiting. However, it must be distinguished from testicular torsion by a physician, often via ultrasound.
3. Incarcerated/Strangulated Inguinal Hernia
What it is: A loop of intestine pushes through the abdominal wall into the inguinal canal and scrotum, becoming trapped (“incarcerated”). Its blood supply can then be cut off (“strangulated”).
Symptoms: Severe groin/scrotal pain, a tender, firm mass in the scrotum that may not be able to be reduced (pushed back in), abdominal distension, nausea/vomiting.
Action: Surgical emergency to prevent bowel ischemia and necrosis.
Part 3: Acute Inflammatory and Infectious Causes
1. Acute Epididymitis (and Epididymo-orchitis)
What it is: Inflammation/infection of the epididymis. Can spread to the testis (orchitis).
Causes:
< 35 years: Typically sexually transmitted infections (STIs) like Chlamydia trachomatis or Neisseria gonorrhoeae.
> 35 years or with risk factors: Typically urinary pathogens (E. coli, Pseudomonas) associated with urinary tract infections or obstruction (e.g., BPH).
Symptoms: Gradual onset (over days) of scrotal pain, swelling, and warmth. Pain may improve with scrotal elevation (positive Prehn’s sign). May have dysuria, urethral discharge, or fever.
Action: Requires antibiotics targeted at the likely pathogen. STI evaluation/treatment of partners is crucial. Differentiation from torsion is critical and often requires ultrasound.
2. Orchitis
What it is: Direct inflammation of the testis. Often viral (e.g., Mumps orchitis), occurring in post-pubertal males 4-7 days after parotitis (swollen salivary glands). Can also be bacterial from spread of epididymitis.
Symptoms: Testicular pain, swelling, systemic symptoms like fever. Mumps orchitis can lead to testicular atrophy and impaired fertility.
Part 4: Chronic and Non-Emergent Causes
1. Chronic Scrotal Pain Syndrome/Chronic Orchialgia
What it is: Unexplained intermittent or constant scrotal pain lasting >3 months. A diagnosis of exclusion.
Potential Contributors: Post-vasectomy pain, nerve entrapment (ilioinguinal, genitofemoral), musculoskeletal pain, or chronic pelvic pain syndrome.
Management: Complex, often involving a multimodal approach: analgesics, nerve blocks (spermatic cord block), physical therapy, gabapentinoids, and psychological support.
2. Varicocele
What it is: Dilation of the veins within the pampiniform plexus (“bag of worms” feel). More common on the left side.
Symptoms: Often asymptomatic. Can cause a dull, aching heaviness, especially after prolonged standing or exertion. May be associated with impaired fertility.
Action: If painful or affecting fertility, surgical ligation or embolization may be considered.
3. Hydrocele/Spermatocele
Hydrocele: Fluid accumulation within the tunica vaginalis. Causes painless, translucent scrotal swelling. Can become large and uncomfortable.
Spermatocele: A cyst in the epididymis filled with sperm. A smooth, round, painless lump above and behind the testicle.
Action: Usually observation. Surgical drainage or removal if large and symptomatic.
4. Trauma
5. Referred Pain
Part 5: The Diagnostic Pathway – What to Expect at the Doctor
A systematic approach is vital. History and physical exam are paramount.
History: Onset, duration, character, radiation, associated symptoms (fever, dysuria), sexual history, history of trauma or surgery.
Physical Exam: Inspection, palpation of abdomen, groin, and scrotal contents. Assessment of the cremasteric reflex and Prehn’s sign.
Urinalysis & Urine Culture: To check for infection (epididymitis).
STI Testing: NAAT tests for Chlamydia and Gonorrhea.
Scrotal Doppler Ultrasound: The key imaging study. Assesses blood flow (to rule out torsion), identifies inflammatory changes, hydroceles, varicoceles, and testicular masses. It is highly sensitive and specific.
Part 6: When to Seek Immediate Medical Attention – The Red Flags
Go to an Emergency Department immediately if you experience:
Sudden, severe testicular pain.
Pain accompanied by nausea, vomiting, or fever.
A testicle that is high-riding, swollen, firm, or has an abnormal orientation.
Scrotal pain following trauma with significant swelling or bruising.
A tender scrotal mass that is also associated with abdominal pain or bloating.
Do not delay. When in doubt, err on the side of caution and get evaluated.
Conclusion: A Symptom Demanding Respect and Urgency
Scrotal pain is a masterclass in clinical triage. It teaches that not all pain is equal—some requires immediate, life-altering intervention, while other causes allow for deliberate management. The responsibility lies with both patients and clinicians: patients must seek prompt evaluation without embarrassment or delay, and clinicians must maintain a high index of suspicion for surgical emergencies like testicular torsion. Through education, awareness, and a systematic diagnostic approach, the serious consequences of scrotal pathologies can be averted, preserving both fertility and long-term health.
Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Scrotal pain can be a sign of a serious condition. Always seek immediate evaluation from a urologist or emergency department for acute scrotal pain